Update 10/22/2021: Don’t buy mouthpiece toothbrushes. Not only do they not work, most of them don’t even turn on. It’s an easy way to get people to send money for scammy things. Need more proof? Go to Electric Teeth at the link below – they have much more current information than you’ll find here.
Mouthpiece toothbrushes: think twice before you buy
IMPORTANT UPDATE 6/5/19: The Amabrush is extinct. This article is useless. Scroll to the bottom to learn why.

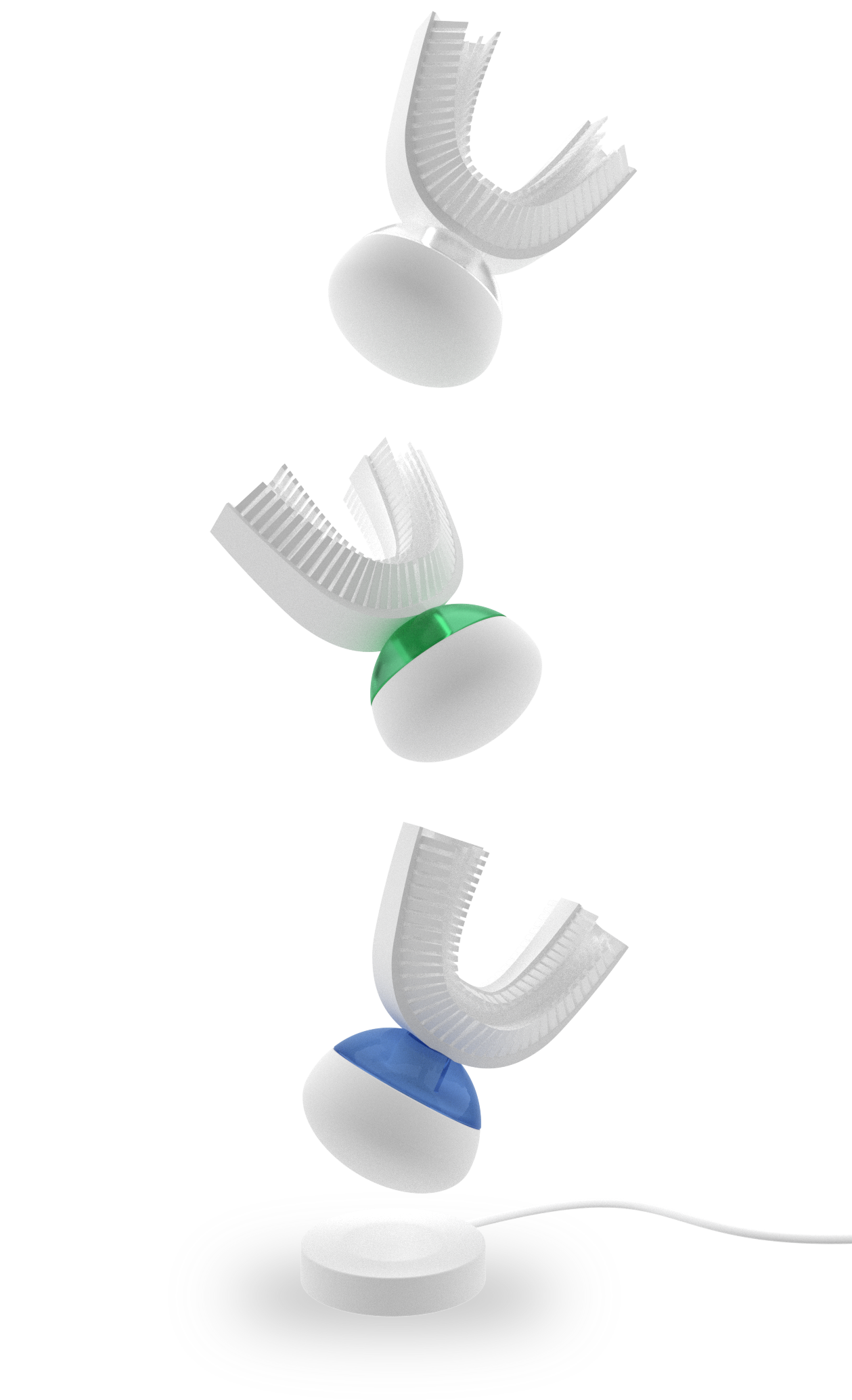
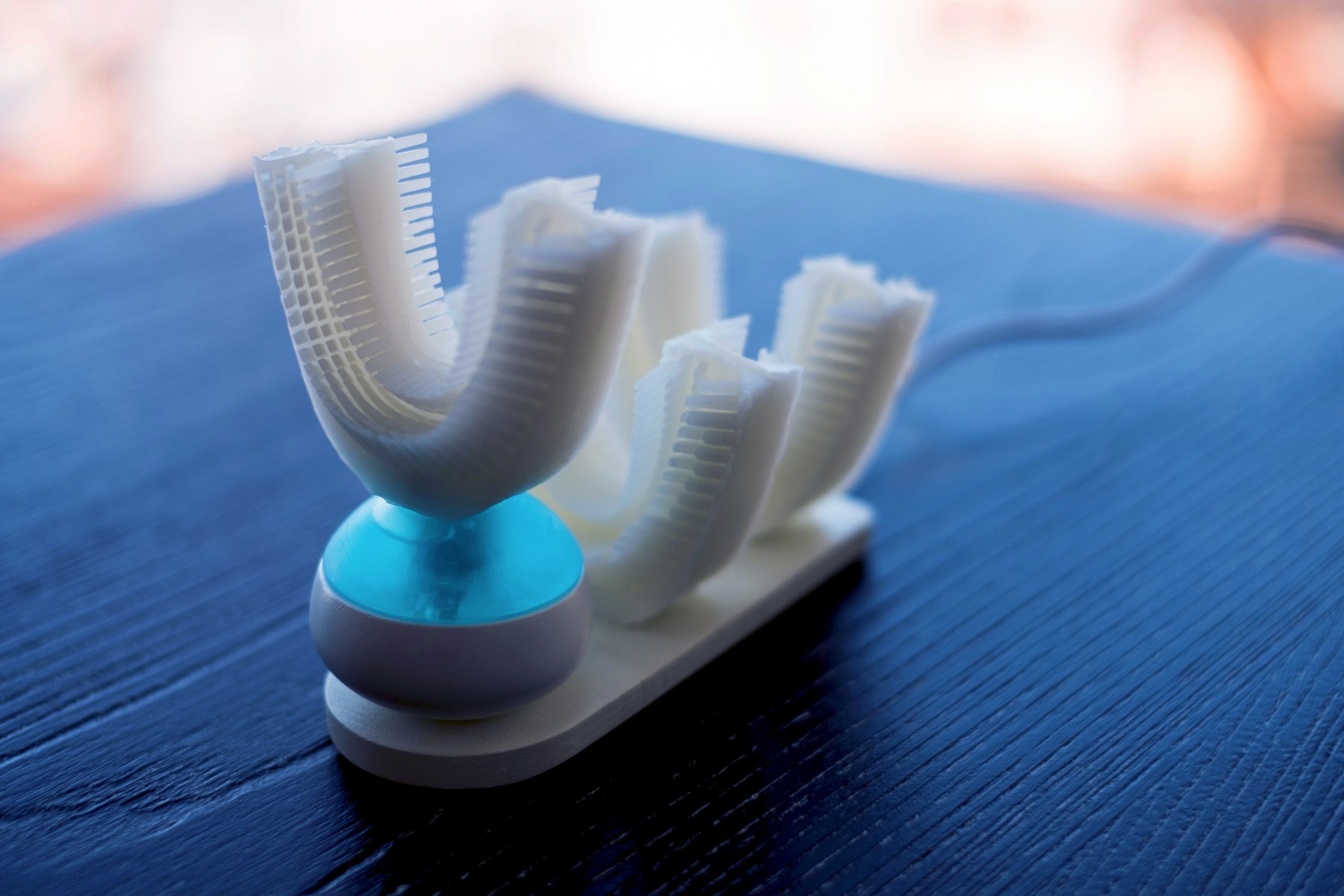
What do you get when you start with a silicone sports mouthguard, embed it with hundreds of tiny bristles, and magnetize a rechargable toothpaste ball that vibrates and cleans all of your teeth at the same time? DentalBuzz recently sat down with the inventor of the new Amabrush to find out where this thing came from, where it’s going, and how to get one.
____
DentalBuzz: Hi Marvin. Thanks for joining us here at DentalBuzz. What’s the story? Tell us about yourself and your company, how you got into the business of toothbrushing, where the name Amabrush came from.
Marvin Musialek: Thank you for having me! Well, my name is Marvin and I’m the founder of Amabrush, a completely redefined toothbrush. I came up with this idea 6 years ago. I brush my teeth twice a day, not because I want to, but because I have to, and this is every dentist’s advice.
 Six years ago I stood in front of the bathroom-mirror as usual, and asked myself, “Why are we on the edge of self-driving cars, but we all still have to stand in front of the mirror and put a stick with nylon-bristles into our mouth, in order to clean our teeth?” Since then I thought about an autonomous cleaning-robot-thingy everyday. Three years later there was still no product like this on the market, and I simply decided to “do it on my own.” I did a lot of research and put a strong team together from many disciplines: dentists, biomedical engineers, physics engineers, electronic engineers and even a psychologist. We had to clarify even the simplest questions with a scientific approach. Why are we brushing our teeth? How should we do it correctly? How much toothpaste? What angle should the bristles have? And so forth. We have been developing Amabrush for the last 3 years and have also received grants from the Austrian Government and the European Commission. With our own money and these grants we were able to finance the cost-intensive development of numerous different prototypes, test-units, pre-production-devices and expert-consultations. Our redefined toothbrush should be seen as a stable and good friend, who takes over an annoying and time-intensive task (toothbrushing) for everyone. So we decided to call it Amabrush, so people who ask “what’s that?” will get their answer: “I’m a brush.”
Six years ago I stood in front of the bathroom-mirror as usual, and asked myself, “Why are we on the edge of self-driving cars, but we all still have to stand in front of the mirror and put a stick with nylon-bristles into our mouth, in order to clean our teeth?” Since then I thought about an autonomous cleaning-robot-thingy everyday. Three years later there was still no product like this on the market, and I simply decided to “do it on my own.” I did a lot of research and put a strong team together from many disciplines: dentists, biomedical engineers, physics engineers, electronic engineers and even a psychologist. We had to clarify even the simplest questions with a scientific approach. Why are we brushing our teeth? How should we do it correctly? How much toothpaste? What angle should the bristles have? And so forth. We have been developing Amabrush for the last 3 years and have also received grants from the Austrian Government and the European Commission. With our own money and these grants we were able to finance the cost-intensive development of numerous different prototypes, test-units, pre-production-devices and expert-consultations. Our redefined toothbrush should be seen as a stable and good friend, who takes over an annoying and time-intensive task (toothbrushing) for everyone. So we decided to call it Amabrush, so people who ask “what’s that?” will get their answer: “I’m a brush.”
DB: Since it doesn’t look like a typical brush, that’s perfect! And endearing. Kind of like the name talks back to you when you say it.
Now, you’re in Austria but also have offices in San Francisco? Before everyone in the United States gets addicted to using your brush, we want to make sure that replacements will be easily available. What percentage of your sales do you see coming to the US once you’re in the retail market?
MM: Yes that’s right. We estimate that 50% of our sales will take place in Europe, especially in German-speaking Europe (Germany/Austria/Switzerland) and the other 50% will take place in North America, especially in the United States. This coincides with our research and as well with our current subscribers, who are also equally distributed between these two regions. Because of that we want to produce Amabrush in these two different regions in the long run.
DB: You have subscribers already? For a product that they can’t even get yet? Okay, so we haven’t even talked about the toothbrush. You’re estimating that its retail price is going to be around $200. While you can’t put a price on good dental health, there have been regular electric toothbrushes in this range for years that have proven not to work any better than the $60 version of the same brand (yes, we’re talking about you, Sonicare). Explain what it is about the Amabrush that puts it far ahead of its competition, and why it is a value at $200.
MM: Yes indeed. We already got 7000 subscribers within a month, which is really, really great. That proves to us that our community is as excited as we are about a toothbrush that takes over the task of toothbrushing. There are many low-priced electric toothbrushes available, but also many high-priced ones. The cost of Amabrush is more to the mid- and high-range, but the brush itself is really high-end. We had to develop everything from scratch, like the micro-pump that foams the toothpaste, the specially formulated toothpaste itself, and the mouthpiece, which was one of the most complicated parts. Not only because we use an uncommon material (anti-bacterial silicone) with a specific toughness, but also because of the integrated, carefully arranged bristles and the micro-channels that deliver the toothpaste directly to the customers’ teeth.
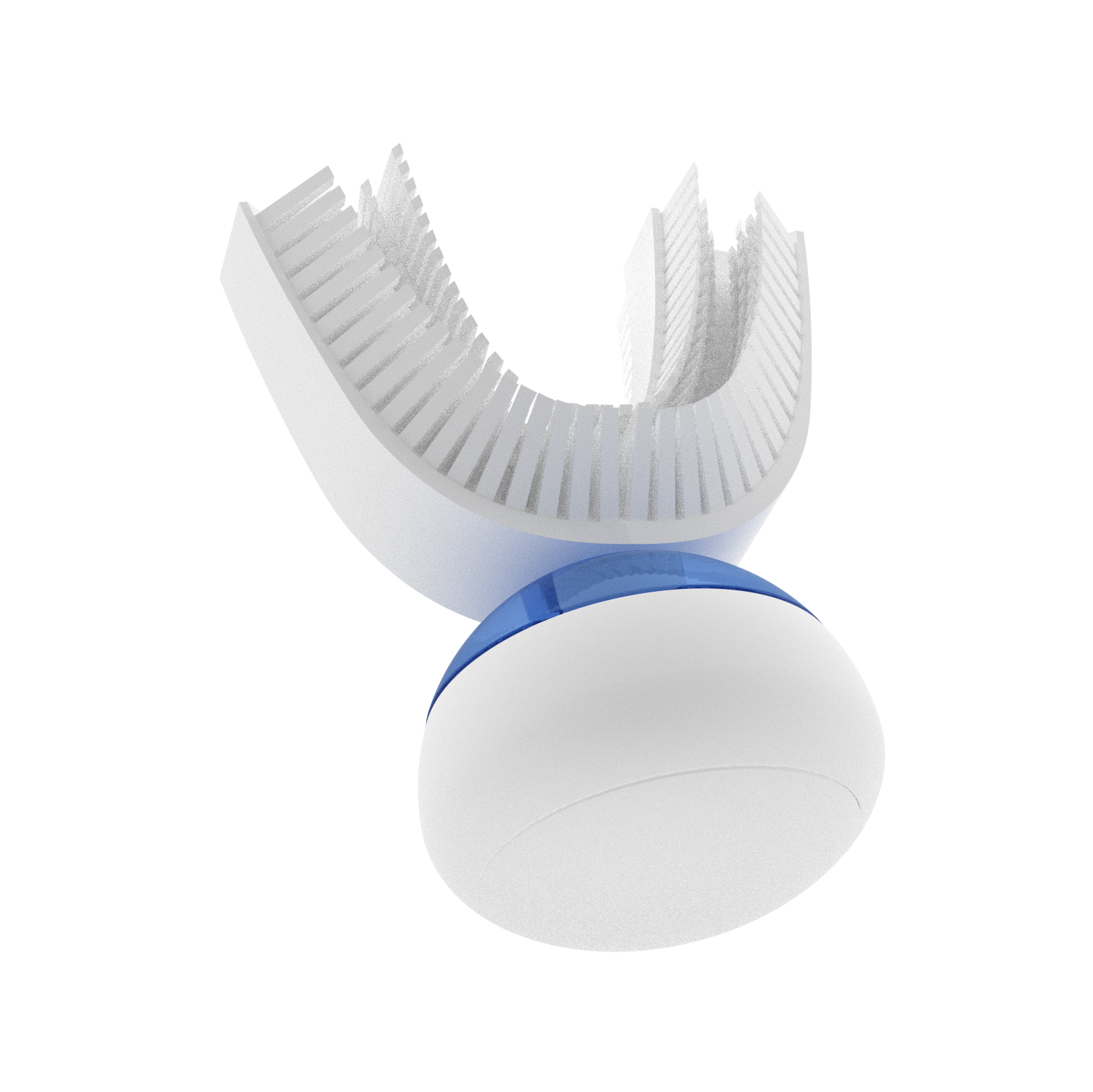
DB: This has the potential to change everything we think we have to do to take care of our teeth. A silicone mouthpiece instead of a handle that you hold as you move a small brush around your mouth, brushing every tooth at the same time, Bass method bristle alignment, self-contained toothpaste, sonic vibrations. If this brush is capable of consistent and thorough plaque removal, then you may have just created the holy grail of preventive dentistry. When and where will customers get the Amabrush once they’re available to the general public?
MM: We have to explain this completely new concept of toothbrushing to people a lot. Amabrush is currently “online-only.” The simplest way for people to inform themselves about Amabrush is over the internet with our online-shop and our website. But in the long run we definitely want to bring Amabrush into grocery stores and drug stores, because the majority of people still buy personal care products “offline.”
DB: Do you see an application for people whose hand dexterity is limited?
MM: Amabrush is definitely also for people with hand disabilities. We developed Amabrush on purpose as a hands-free device, not only that it is as convenient and automatically as possible, but also that there is no barrier in order to use it.
DB: What does it feel like to use?
MM: It feels like if someone else brushes your teeth with a soft bristled toothbrush paired with the feeling of a gingival massage.
DB: So it’s sort of like having your teeth cleaned by a professional? We would imagine that would be pretty effective. What kinds of plaque index scores are you getting; in other words, how well does the Amabrush actually clean compared to manual or other electric toothbrushes?
MM: That’s true, it does a pretty good job at cleaning your teeth! We’ve had plaque index scores calculated by an independent clinical institution and have been pleased with the results. What’s worth knowing is that Amabrush is not necessarily better than a regular manual or electric toothbrush, because common toothbrushes work good enough if they are used properly. The thing is, Amabrush is way more convenient. You can do so many things wrong with a regular toothbrush, as you have to be highly concentrated for at least 120 seconds each time you brush your teeth. And while brushing, you should use different methods like the Bass method paired with the red-white technique. This is not only time-consuming, but also annoying for most people. Because of this, people usually tend to do something else while brushing their teeth. Furthermore, they put too much pressure on the toothbrush which can damage their gum. What’s more, most of the people don’t brush their teeth long enough. Amabrush cleans your teeth the same every time, with the right technique, and does not depend on your concentration.
DB: What it sounds like you’re saying is that the problem with electric toothbrushes is that manual ones are just that – they have to be moved around with your hand, so even if they’re the best at what they do, they’ll still miss areas because the human being attached to the hand doesn’t apply the brush properly. The Amabrush provides hands-free brushing at a fraction of the time? Very novel.

Back to your subscribers, then. How can subscribers order the Amabrush? How can I get one as a consumer? What do I need to do?
MM: Interested customers can subscribe to our newsletter right now on our website. We created a landing-page that explains all relevant information and details about Amabrush and the upcoming Kickstarter campaign. Speaking of which, this will be the first opportunity for our customers to get Amabrush. We will start our crowdfunding-campaign on Kickstarter next week (end of June 2017). Customers have the ability to support our project, and as a return, get Amabrush at a strongly discounted price ($69 instead of $199)!
Regarding your question what the customer needs to do: simply sign up for our newsletter on our website (www.amabrush.com). We will send a reminder with the exact date of our Kickstarter-campaign to all subscribers. When the campaign is live, simply choose a package that suits best for you. All of them are strongly discounted, as this is our way to say “Thank you” to all of our supporters and the community!
DB: Dentists and dental hygienists are particularly interested in finding new ways like yours to pass on to our patients that help them keep their mouths healthy. Do you have anything more you’d like to say to us?
MM: Our pre-production units are already in the making, in order to be shipped around the globe to various dentists. We highly appreciate feedback and input from every professional expert in order to make Amabrush as perfect as it can be. We are really looking forward to the support of our community!
DB: Thanks again, Marvin for sharing your story with us, and we sincerely hope that you get all the attention that this Kickstarter campaign deserves.
MM: We hope that too. Thank you very much for the interview and the great time!
![]()
UPDATE 6/28/2017: Amabrush announced today that the launch date for their Kickstarter campaign is next week – July 5, 2017.
UPDATE 7/5/2017: The campaign is now live, with the Amabrush expected to begin shipments in December 2017. This video shows close-up vibrations of the prototype. We imagine that the production version will be even more refined.
Many patients took part in our dental studies, which took place on 3 different dates with a minimum interval of 24 hours. The tests were performed and evaluated by independent dentists. Amabrush was tested simultaneously with two different institutions and two different sets of patients.
The TQHPI (Turesky modified Quigley Hein Plaque Index) which we used as the method determines how much plaque was present on the teeth – the lower the value, the less plaque on the teeth.
Test procedure
1.) 24 hours before the test, participants were not allowed to brush their teeth. For the plaque test, the patients chewed plaque disclosing tablets so that the dentist could then determine the initial plaque values (tablet is used to make plaque visible).
2.) Patients had to brush their teeth with a regular manual toothbrush for at least two minutes. The remaining plaque values were determined afterwards.
3.) The same process was repeated for the second appointment one week later, but this time with using the Amabrush instead of the manual toothbrush. Teeth were cleaned for just 10 seconds and the dentist determined the plaque values again.
Results
The plaque index decreased statistically significant and there was no statistically significant difference between Amabrush (with 10 seconds brushing time) compared to a regular manual toothbrush (with roughly 3 minutes brushing time on average).
These results make us truly proud and show us that hard work, clever engineering and patience pays off for all of us. We hope that you also like those results, which we would have never reached without your support, help, and feedback!
Images courtesy of Amabrush™ All rights reserved. This article has been written with no bias towards compensation or commissions. DentalBuzz stories run on ideas, not pay-per-clicks.
Want to know when we post a detailed review of the Amabrush once it’s available and we’ve had a chance to chomp on it? Be sure to subscribe to DentalBuzz by adding your email address and you’ll automatically get notifications each time we add a new article.
FINAL UPDATE 6/5/19: Nevermind. Amabrush is officially done. No surprise there, unfortunately, because they’ve been propping up their company with delays for the last two years. Here at DentalBuzz, we never even received our super early bird Amabrush. What’s worse though, is our role in this for convincing our readers to invest in the Kickstarter campaign. At this point, we feel sort of like everyone who invested in Theranos, with their fake blood testing. Great ideas still depend on that which is physically possible, but Marvin still doesn’t seem to get this! You can read the litany of excuses here from Amabrush: https://www.amabrush.at/blogs/news/important-information-regarding-amabrush-company. Bottom line? We’re sorry, and you still have to brush your teeth for two minutes.

 Toddler-friendly? Check again.
Toddler-friendly? Check again.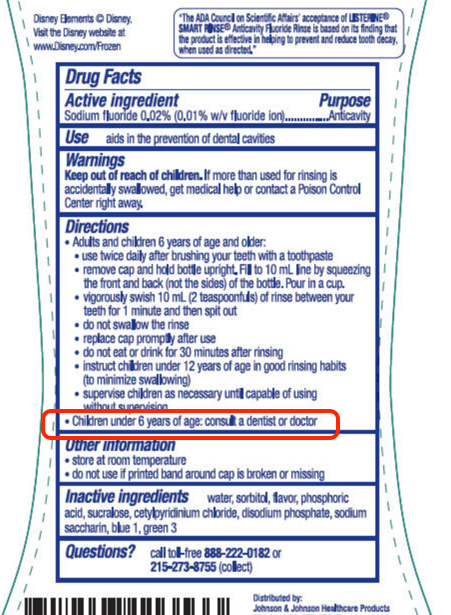
 • What do all ACA-qualified plans have in common with each other? At the very least, every insurance policy must include fluoride supplementation at no cost for children under age 5. Supplements are recommended mostly in areas where the fluoride level in water supplies are inadequate, and age five and below is the time frame when teeth can be protected most by the ingestion of fluoride. The supplements can be in the form of drops, chewable tablets, or as combination vitamins. All fluoride supplements require a prescription, either from a dentist or a physician’s office.
• What do all ACA-qualified plans have in common with each other? At the very least, every insurance policy must include fluoride supplementation at no cost for children under age 5. Supplements are recommended mostly in areas where the fluoride level in water supplies are inadequate, and age five and below is the time frame when teeth can be protected most by the ingestion of fluoride. The supplements can be in the form of drops, chewable tablets, or as combination vitamins. All fluoride supplements require a prescription, either from a dentist or a physician’s office.


 A blogger since 1997, Trish Walraven, RDH, BSDH is a mom and practicing dental hygienist in the suburbs of Dallas, Texas. Her mission with DentalBuzz is to offer a fresh podium of discourse for those involved in dentistry and to expose fun in our professional lives.
A blogger since 1997, Trish Walraven, RDH, BSDH is a mom and practicing dental hygienist in the suburbs of Dallas, Texas. Her mission with DentalBuzz is to offer a fresh podium of discourse for those involved in dentistry and to expose fun in our professional lives.