We love sharing good information that empowers dental practices to make unbiased decisions, which is why our friends at SoftwarePundit didn’t even have to send us any sort of payment, contactless or otherwise, to get the word out about their dental software review site. This category of solutions should be on the top of your research list right now, for obvious reasons.
by Bruce Hogan

Traditionally, dental practices have been slower to adopt new technology than other medical practices. Most dental professionals can understand why – implementing new technology is a time consuming and tedious process! However, the benefits of overcoming these barriers are often well worth the pain. Do you remember the days before automated appointment reminders? Without software tools, front-office staff were forced to manually call patients before every appointment!
Practices nationwide are increasingly adopting payment processing technology called contactless payments. Contactless payments refer to a variety of ways that patients can pay for treatments digitally, whether it’s paying through a text message or using a mobile wallet like Apple Pay. Patients are no longer forced to pay by mailing a check.
Why are dental practices starting to offer contactless payments? It’s what patients want! A recent study showed that 35% of customers are interested in paying with a text from their phone, but only 4% of small businesses offer this payment option. Additionally, 62% of buyers under the age of 35 would frequently or always pay with a text from their phone if they could. Allowing patients to pay the way they want to is an effective way to increase revenue and patient satisfaction.
Covid-19 is accelerating the need for dental practices to adopt payment technology. With shelter-in-place orders, patients can’t physically come into your office to pay for treatment they have received. Many practices are understaffed or closed right now, and do not have the capability to print and mail statements. Most importantly, when patients do begin returning to practices, contactless payments will allow patients to pay without any direct physical contact with your team.
Benefits of Contactless Payments for Dental Practices
There are three primary benefits of contactless payments: they lead to improved operational agility during crises like coronavirus, increased revenue, and reduced administrative workload.
Contactless Payments are Particularly Beneficial During Coronavirus
Contactless payments are ideal during Covid-19 because it allows patients to pay for treatments without being physically close to staff. Practices can use contactless payments to collect payments for services they have rendered prior to the shut down. This would be especially beneficial for cash-strapped practices that need an immediate influx of cash.
Additionally, contactless payments could be a part of the operational changes that practices make to increase safety after reopening. Contactless payments allow patients to maintain a safe distance from front-office staff when making payments. It’s congruent with the social distancing behavior that we’ve been practicing since March.
Finally, contactless payments are a valuable tool for practices that offer teledentistry appointments. After appointments are finished, you can immediately send patients a payment request digitally. This makes the payment process much easier and faster for both parties.
When practices offer patients more options to pay, they pay more often
Weave, a patient communication software company, commissioned an independent market research firm to survey a random sample of 380 small business customers and 350 small business owners to understand their behaviors and perceptions regarding payment options. In this study, the research firm found that small businesses that offer more payment options increased revenue by 29%. The study’s conclusion supports a common sense notion that we, as consumers, can all relate to – we are more likely to pay, if we can pay the way that we want to!
Contactless Payments Makes Billing Easier for You
Contactless payment software also reduces a lot of clerical work for dental practices. Traditionally, the collection process involves printing and mailing statements, entering billing information, and managing merchant accounts. Most contactless payment software automates these tasks for you. For example, the billing process using Weave’s text-to-pay feature involves a single text. The patient inputs their own payment information, and the software automatically processes the payment.
Types of Contactless Payments
There are several types of contactless payments. While they differ slightly, all share the benefit of patients being able to pay remotely.
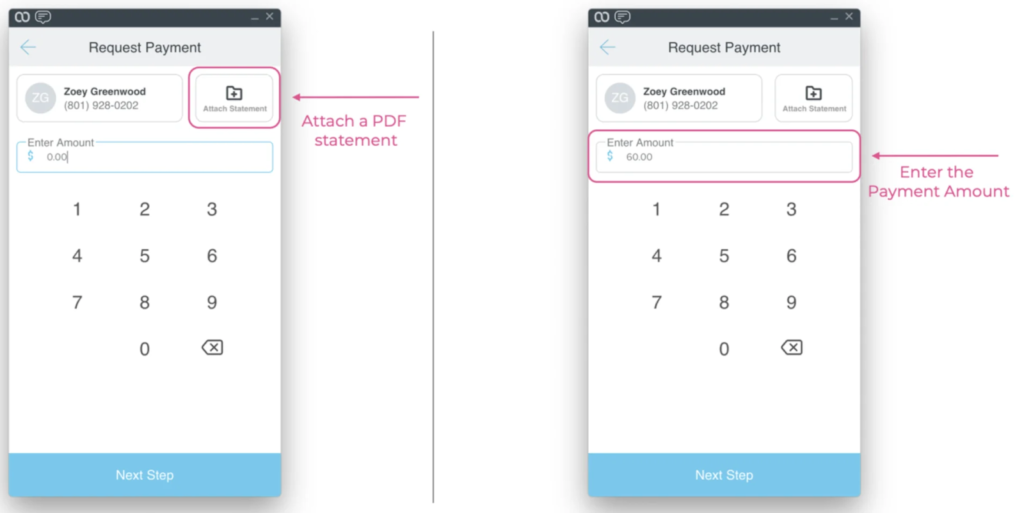
Send Payment Requests by Text
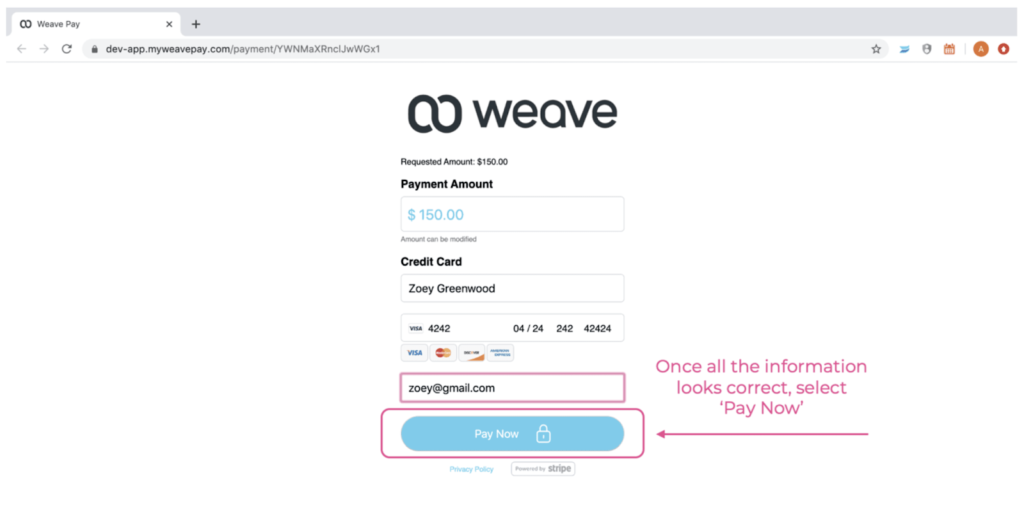
Practices can use software tools, like Weave, Podium, and Doctible, to send payment requests by text. You simply enter the patient’s phone number, input a treatment amount, and attach a statement. This is much easier than traditional collection methods that involve printing and mailing statements, collecting billing information, and charging each transaction manually! Patients input their own billing information into the text, payments are automatically processed, and the money goes straight into your bank account.
Send Payment Requests by Email
Many software tools allow you to send payment requests by email. The process is similar to sending payment requests by text. You enter the patient’s email address, attach statements, and enter payment amounts. The software takes care of the rest.
Process Payments with a Desktop Application
For patients more comfortable paying for treatment over the phone, many solutions have desktop applications with a payment-processing tool. Front-office staff can input card information directly into the app, and the tool automatically processes the payment.
Receive Payments Through Mobile Wallets
Many patients prefer paying for treatment using a mobile wallet, like PayPal OneTouch and Apple Pay. Making this payment option available makes the billing process more convenient for your patients.
How to Get Started with Contactless Payments
Here’s a list of steps that we recommend when searching for the right vendor. Typically, the process takes about 1-2 months from initial research to completed software implementation.
- Create a Short-list of Potential Vendors
Make a list of the vendors in the market that interest you. We recommend Doctible, Podium, and Weave to get your list started.
- Research Each Vendor
While doing your research, keep an eye out for the most important qualities in the vendors. This includes price, features, and quality of customer service. SoftwarePundit provides in-depth analysis on many vendors that provide contactless payments. Check them out!
- Talk to Existing Customers of Each Vendor
One of the best ways to learn about vendors is to speak with customers who have used the product first hand. Customers will typically speak candidly about what they like and dislike about the product, and give you a clear idea of what you should expect. SoftwarePundit for Dentists is a Facebook group created to serve as a platform for dentists to discuss dental software.
- Go Through Sales Process
Reach out to each vendor, and begin the sales process. The sales process typically involves a series of steps including:
- Introductory call
- Product demo
- Product testing
- Contract negotiation & signing
- Software implementation and staff training
Are You Ready to Find The Best Software for You?
Finding the right software to implement contactless payments can be a confusing process. Our job at SoftwarePundit is to make this process easier, and help you pick the best software that fits you and your team’s style and needs. Come visit our website if you have any questions about contactless payments in dentistry!


Bruce Hogan is Co-founder & CEO of SoftwarePundit, a technology research firm that provides advice, information, and tools to help businesses thrive. Bruce has experience investing at multi-billion dollar private equity firms, leading teams at venture-backed Internet companies, and launching new businesses.




 Do you know how sometimes, when you get a new piece of equipment, it’s so Shifta La Paradigma that you can’t even THINK about working without it? You get a little anxious about the possibility of it failing and having to go back to the old way of doing things. What do you do?
Do you know how sometimes, when you get a new piece of equipment, it’s so Shifta La Paradigma that you can’t even THINK about working without it? You get a little anxious about the possibility of it failing and having to go back to the old way of doing things. What do you do? Opinion #2: Cords are better. And worse.
Opinion #2: Cords are better. And worse.


