As someone who has been a dental hygienist for over 30 years, and who has personally worn through a drawerful of nightguards, I feel a bit qualified to get a little judgy about whether a nightguard that bypasses the dental office has any real value, is safe to wear, and is actually a reasonable alternative.
How did this even catch my attention?
If you’re like me, your social media eventually figures out what you do for a living and starts targeting you accordingly. A few months ago, mine decided I needed a new nightguard. And honestly, at this point in my life, the algorithm was not entirely wrong.
When I was fresh out of college, the first dentist I worked for pointed out that I had significant wear on the incisals of my canines, especially. I believe his exact sentiment was that what he was seeing was not the teeth of a typical 23-year-old. More like someone in their 40s. Ouch, my vanity did not like that.
That was enough for me to realize I did not want to arrive at my later years with a flat, worn smile with no personality, and a profile where my nose and chin were closing in on each other. So I had my first impressions taken and a lab-made nightguard fabricated, and I have worn one ever since. One of the perks of working in a dental office is that you usually only pay lab fees for appliances like this, which means I have had access to high-quality dental appliances at very good prices for decades.
Fast forward to now. While I’m still a licensed dental hygienist, I am not currently working chairside, which means those perks are gone. So when I started seeing those ads for online custom nightguards, I started clicking on a few.
I ended up at JS Dental Lab (https://jsdentallab.com/) after deciding that theirs seemed the friendliest company to investigate. When I reached out and explained that I write for DentalBuzz, the owner offered me a complimentary nightguard so I could review it. Even though my device was delivered to me at no cost, I went through the same process to get it that any patient would.
Their website walks you through a decision tree to select your guard. Because I am a heavy bruxer, I picked the most badass option they had, which was their Premium 3D 4mm Hard Shield. And when it arrived, my first thought was… this is pretty dainty. Especially compared to the majority of the nightguards I have had in the past. The fit was also different in that there was a higher coverage depth, so the online nightguard covers more of the facial (front) of the teeth.

Why online nightguards might be thinner
This is where it gets important. Online labs have to be conservative. They are not seeing you in person. They are not checking your bite or making adjustments chairside. So they cannot risk making something too thick or too aggressive. If they did, the nightguard then technically becomes a splint, which is a medical device that could cause real problems like:
- teeth shifting
- supereruption
- bite changes
- TMJ issues
So yes, the online nightguard is thinner than the dentist’s splint in the top image. Noticeably thinner. But that is intentional. They are trying to give you something to grind on without creating new problems. An in-office nightguard is part of a process. It gets checked, adjusted, and followed up on. An online nightguard is a finished product that shows up in the mail and is not as easy to fine tune.

The Biggest Challenge: Taking your own impressions
Here is the part that matters the most: taking your own impressions is hard. Even for me. I spent years making whitening trays for patients. I was very comfortable with alginate. Give me a tray and some pink goo and I was happy all day. I loved pouring the models, waiting until the tray material melted enough to quickly suck it down over the plaster.
This is not that.
The silicone putty they send for you to mix together is different, and getting a clean, accurate impression on yourself is a completely different experience than doing it on a patient, especially if you slobber a lot. In my opinion, JS Dental Lab does everything right on their end:
- multiple tray sizes
- extra silicone putty in case you mess up
- clear instructions
- no-cost remakes if needed
But still. It took me a few tries to get it right. And that is the biggest limitation of this whole model. Everything depends on the impression.

We have already seen what happens when dentistry tries to go fully remote. Remember all the marketing a few years ago with “do it yourself” orthodontics? SmileDirectClub started with a lot of promise and ended up being a lesson in what happens when business scales faster than clinical oversight. Whoo boy. If you’re up for a little side quest, DentalBuzz originally began snarking about SmileDirectClub in 2014, where you can check up on the latest update that includes a newly posted video documenting their demise.
Now, nightguards are not changing your teeth. They are much lower risk. But the same basic truth applies. Dentistry works best when someone is actually looking at your mouth.
So… Are They Any Good?
Yes. With caveats.
I would recommend an online nightguard if:
- cost is a concern
- you just need protection from grinding
- you are willing to deal with the impression process
- you understand it may not last as long
JS Dental Lab, specifically, does a really good job with:
- overall customer service
- remakes and adjustments
- covering shipping both ways
- using materials that are comparable to what you get in a dental office
When it comes to the actual nightguard I received from JS Dental Lab, I don’t have anything to criticize about its quality. The acrylic looks and feels identical to every dentist-made appliance I’ve had over the years. It’s comfortable, stays in all night, and comes out easily in the morning, which is really all I need it to do. And I will say, the case is a nice upgrade. Sleek, silicone-lined, magnetic close. A noticeable step up from the usual retainer cases that dental offices buy in bulk.
You should go to a dentist instead if:
- you have any pain at all
- you suspect TMJ issues
- you want something that will last longer
- you gag easily
- you do not want to deal with impressions
The digital scan alone is a huge advantage.
For dental professionals: what do you tell your patients?
Because they are going to ask.
Here’s the answer I’d give:
If a patient with bruxism just needs something to keep them from grinding their teeth down into a flat plane, an online nightguard is a perfectly reasonable option. Especially if cost is the thing standing between them and doing nothing at all.
If there’s pain, joint issues, headaches, bite changes, or anything even hinting at TMJ disorders, they need to stay in the dental office. Full stop. If they want something thicker, longer-lasting, and actually adjusted to their bite, that’s also a dental office situation.
But if it’s truly a choice between some protection vs no protection, I’m picking protection every time.
And one last thing, because it always comes back to this: aesthetics, the quiet fear of aging too soon, and the weight we carry around how our faces change over time.

Bruxism slowly files our teeth down, which quietly steals a little vertical dimension over time. And when that space goes missing, the lower face doesn’t just shrug it off. It settles. Compresses. Gets a little… creased.
Right where your lipstick betrays you by bleeding into those little cracks.
I’m not saying a nightguard is the new anti-aging miracle. I am saying that keeping a little height between our teeth over the years seems to work in our favor.
All these years in, I like my odds.

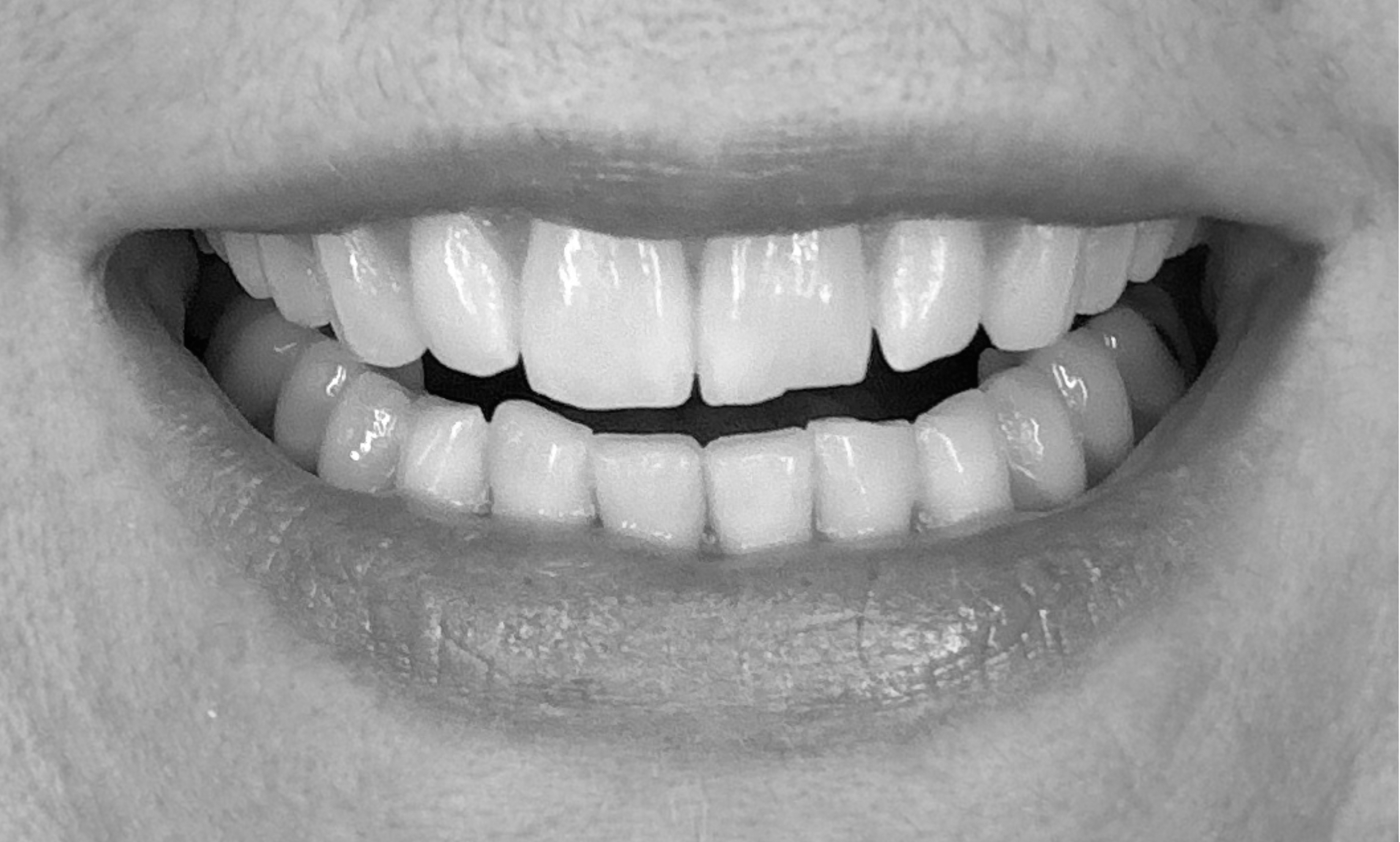
Trish Walraven, BSDH, RDH is a dental hygienist with a lifelong habit of taking her stress out on her teeth at night. She figured she’d go ahead and offer closeup photographic evidence after deciding that, for someone approaching her sixth decade, it could be worse.
References & Further Reading
- JS Dental Lab Website: https://jsdentallab.com/
- Occlusal splints and bruxism management (ScienceDirect review Comprehensive review of how nightguards (occlusal splints) are used to reduce tooth wear, muscle activity, and protect the dentition.
- Clinical overview of occlusal splints and TMD treatment Explains how nightguards are used for bruxism, TMJ disorders, and stabilization of the bite, including their role in maintaining vertical dimension.
- How occlusal splints protect teeth and reduce grinding damage General clinical explanation of how nightguards act as a protective barrier and reduce symptoms like jaw pain and headaches.
- Unintended bite changes associated with nightguard use (BDJ review) Discussion of how poorly designed or unmonitored appliances can lead to occlusal changes, reinforcing the value of professional oversight.
- Digital vs traditional splints and fit accuracy (clinical study) Shows how digitally fabricated appliances can improve fit and consistency, supporting the advantage of in-office scanning.
- Effects of occlusal splints on vertical dimension and muscle activity Demonstrates that splints can increase vertical dimension and reduce muscle hyperactivity, which is directly related to both function and facial structure.








 freelance writer for the health care and financial services industries. As a stand-up comedian on the side (and after the right amount of drinks) she aspires to bring comedy to her writing while providing useful information for her readers.
freelance writer for the health care and financial services industries. As a stand-up comedian on the side (and after the right amount of drinks) she aspires to bring comedy to her writing while providing useful information for her readers.