What in the phôc is Phocal? The name is oh-so-clever, the way it changes up the F-sound, pinpoints the precision of its delivery mechanism, adds in a little calcium and acid/base interplay there. Plus, the little disks sorta kinda look like contact lenses. Phocal – the latest in fluoride therapy.

Of course! It’s because they haven’t been DentalBuzzed yet.
The few articles that I’ve read about Phocal so far are as exciting as your average WHAT’S NEW IN DENTISTRY dreck. DentalBuzz is here to change that, to present to you all the facts about Phocal Therapy in an entertaining, yet insightful package designed to bring the maximum exposure possible to a product that will sink or swim on its own merit in the end.
Problem #1: Incipient interproximal lesions
If you’re not in dentistry you probably don’t know what these are. Let’s just call them future “Cha-Ching!” You know when dentists take radiographic images inside your mouth with x-rays? They’re looking for cavities between your teeth, where sugar and decaying bacteria ferment into acids that dissolve the surface of enamel into a mass of tiny swiss-cheese chalky goo.
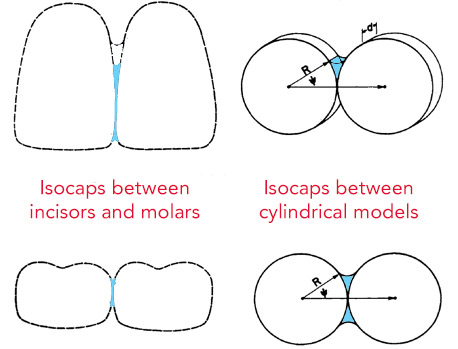
Problem #2: Isocaps
Even many dentists have forgotten what an isocap is, so that’s why I’m going to explain them to you and why a Phocal disk inhibits their formation. Essentially an isocap is a bubble created between two flat surfaces that prevents liquids from wicking into it. Isocaps have to do with capillary action and surface tension.
The Solution: Jam Some Stuff Between Your Teeth
If you can’t penetrate an isocap, well then, just obliterate it, take it out of existence, displace it. Whatever it takes, just put something ELSE there. Fluoride has been proven in many studies to increase the remineralization of a tooth that has begun to weaken, which is why fluoride is the active ingredient in the Phocal disks.
I’d explain how this whole process works, the options available, and even the studies that show how Ah-May-Zing this new fluoride therapy is except that someone at Collident paid a production company to make this perky animated video that does the job for me pretty well. Yes, you DO have three minutes to watch it. And there’s no voice-over, so feel free to turn off your sound before you click the arrow to start it up.
The Obstacles: Price, Chair Time and FDA Approval
What…you were expecting that these disk are THE answer to cavities between our teeth, forever and ever, end of discussion? If they were perfect we’d all have them in our mouths right now. For one thing, they’re not cheap: a box of 20 Phocal disks cost the dentist around $125 – that’s over $6 for each insertion. And because they are “technique sensitive” (read: only an experienced professional can place them) you’ve also got to deal with the dental office overhead fees. As far as the FDA approval goes, as of the time of this publication it appears that the Food and Drug Administration says that the Phocal Disc is unapproved, stating “this drug has not been found by the FDA to be safe and effective, and this labeling has not been approved by the FDA.”
Does this mean, then, that Phocal disks are doomed to obscurity and demise? Not necessarily. Dentists have no problem purchasing a box from the usual channels, but they may not be aware that this therapy exists in the first place, because there are all these flashy things in dentistry that many dentists prefer to spend their time learning about besides prevention. Besides, there’s more money to be made by fixing decayed teeth versus trying to preserve demineralized ones. That’s why the 5th dentist never recommends sugarless gum to his patients who chew gum (!). Cavities keep dentists profitable.
Which is why it’s now YOUR job to ask for Phocal disk therapy the next time your dentist wants to “watch” a spot between your teeth. And that is because watching is a very, very unhealthy type of voyeurism in the dental world.
![]()
References:
University of Michigan: Capillary Action around Dental Structures
National Library of Medicine: http://dailymed.nlm.nih.gov/dailymed/Phocalfluoride
 You’d better pre-order soon, though. As soon as the FDA and other authorities get wind of this there will be an immediate shutdown of all shipments. You know how good our government is at shutdowns. Product is supposed to begin its journey to the US tomorrow if it all goes as planned, however.
You’d better pre-order soon, though. As soon as the FDA and other authorities get wind of this there will be an immediate shutdown of all shipments. You know how good our government is at shutdowns. Product is supposed to begin its journey to the US tomorrow if it all goes as planned, however.