
Not long ago, all dental practices were owned by the dentist who took care of you. Sure, they might not have given you any anesthetic before they smashed silver crunchy metal into your cavities, and they may have slapped you around and given you Post Traumatic Stress Disorder any time you thought about opening your mouth wide for anyone, but at least you knew that the dentist shoving their knuckles into your nostrils was the one dictating how things were done around there.
Since then, dentistry has gone all Wal-Mart on the public. There are thousands of dental offices that are part of large chains, where the dentists who take care of you are merely employees, where the quality of dental care provided to patients is secondary and instead the amount of profit generated by each provider becomes the indication of that person’s worth within the company. Can you imagine a leaderboard, like in a sales department, where all the dentists’ production numbers are on display for the entire office, so it’s a race to see who can make the most money?
As a patient, don’t you get giddy at the thought of being ridden like a thoroughbred horse? Me neither. My health is not a commodity.
Dentistry is a little different creature than regular medicine in the sense that TEETH ARE OPTIONAL. You can be a very healthy individual, only with no teeth. It’s kind of like having a hand amputated – your quality of life may be affected, but a hopelessly infected hand should be removed and replaced with a prosthetic. If your body is rejecting your teeth for whatever reason, that’s when there are health concerns as well. Dental professionals make it their life’s work to help you keep your teeth in as close to original condition as possible.
The problem is that when money is involved, you can bet that there are those who will abuse this relationship. There’s scare tactics, there’s bait-and-switch, there’s all the usual sleazy sales pressure used to extract as much income from each patient as possible. New patients often bring us treatment plans that they are unsure of, looking for second opinions, trying to figure out why they don’t trust the previous dental offices’ diagnoses. I just want to say it straight, “They’re taking you for a ride, dear.”
Whip. Whip.
Well crud, I never wanted this article to be an analogy of horse racing with the big hats and Bourbon and milk-drinking and jockeys. So, let’s start over and begin talking instead about Red Flags and Grey Areas.

Red flags, of course, are the signals you get when you realize something that seems good, isn’t so good. Red flags are big fat warning signs.
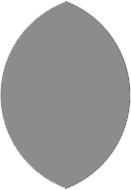
Grey areas, are, well, not really black and not really white. Grey areas are where black and white kind of blur into each other, and sometimes they end up looking a little suggestive (!) like the image above. Yeah, sorry about how weird that looks when I take it out of context.
When it comes to the health of your mouth we usually look at two things: your teeth, and the stuff that holds your teeth in your mouth. That’s what we’re going to talk about in this discussion, what you think of as your gums. Dental professionals call this part of you your periodontium. If your gums are in excellent condition, you have what is called periodontal health. On the other hand, if your gums are seriously letting go of your teeth you have periodontal disease.
As you can see, the biggest part of this diagram is the Grey Area. This is where most people land, especially if they haven’t been to the dentist in a while. Even if your front teeth are mostly healthy often you’re automatically categorized into the Very Diseased category because you have too many spots in your mouth that are infected with bacteria to treat you as a Very Healthy person. That’s when you’ll get a treatment plan designed to minimize the effects of your disease.
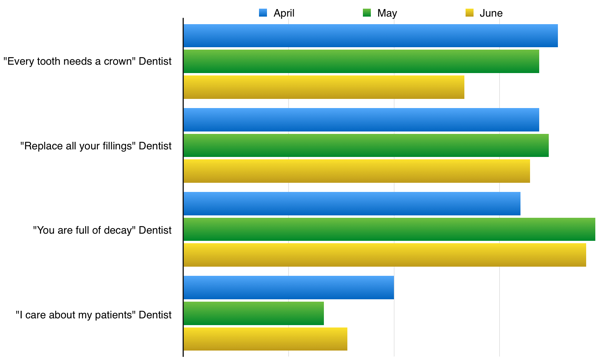
When your mouth is in the Grey Area, this is where treatment recommendations can vary the most from office to office and even from person to person. Almost every dentist will prescribe the same treatment course if your case is black and white (very diseased or very healthy). If you’re in the Grey Area though, this is when Red Flags will start to stick out.
There’s one Red Flag in particular that keeps showing up. Arestin® is a yellow powder containing minocycline microspheres – an antibiotic designed to help diseased gums heal faster. The powder is puffed deep into an infected spot under the gumline where it hardens upon contact with moisture and time-releases the antibiotic for about three weeks. Here’s what the package of cartridges looks like, with the yellow powder in the tip:

Arestin is a great product! I’ve seen stubborn gum disease completely disappear when we’ve used it very selectively in our practice. So the Arestin itself isn’t a problem. The problem is how it’s being prescribed.
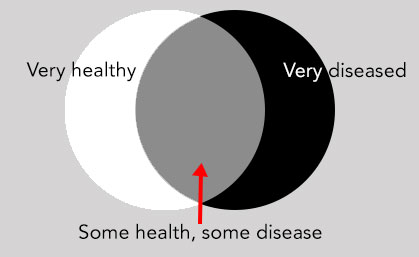
Say you had your gum disease treated with scaling and root planing (a “Deep Cleaning”), but a few spots are still unhealthy a month or two or three later. If your dentist or hygienist sees that you still have open sores that are higher than a certain parameter (over 4mm is considered the standard) this is when Arestin therapy provides the most benefit.
So when is Arestin a Red Flag? You’ve visited a new dental office, and not only are they recommending that you have treatment for your periodontal disease, they’re also saying you need a course of Arestin to be placed on the same day that you have your initial treatment. It’s even a bigger red flag if you floss regularly and never see your gums bleed.
The thing is, Arestin isn’t cheap. Just a single cartridge costs your dentist upwards of $15. Then there is the insertion fee; in other words, what the patient is billed for placement, and than can run as much as $60 per site.
Here’s where it gets crazy. An average mouth has 28 teeth. Each of your teeth has as many as six sites where Arestin can be placed. Let’s see, that’s $90 in material costs, $360 in placement costs. That’s potentially going to cost you $450 – per tooth.
You’re seeing the big picture now: treating gum disease can be quite profitable! This is why Arestin is such a big deal in the offices that are part of corporate dental chains designed for maximum shareholder profit. This antibiotic is marketed to dental professionals as a way to help us make money, all in the name of “helping our patients.”
So how do you end up getting prescribed Arestin therapy if your mouth is pretty healthy? If your hygienist or dentist was instructed to “force the probe” to create a deep measurement, that’s how. Stab ’em hard and voila! Fake gum disease! Here’s a story that exposes some of the bad things that have allegedly happened in corporate dentistry, including this example:
http://www.pbs.org/dentalworks-chain-misdiagnosed-for-money-dentists-say/
As you can see, lots of other stuff can be exaggerated as well to make sure that the dentistry performed on you is as profitable as possible. For now, though, we’ll stick to talking about the Red Flag, because this one cue may help you decide whether or not you’re being over treated.
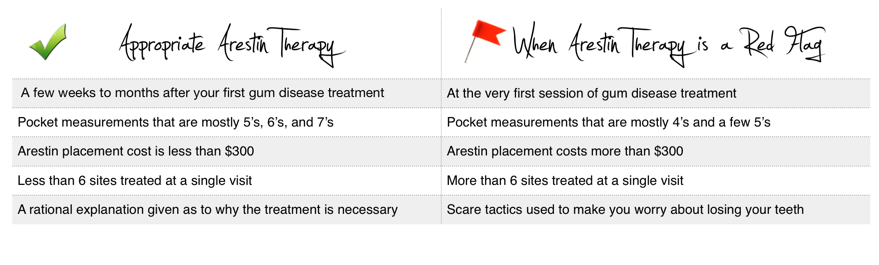
Here are the professionally accepted general guidelines about Arestin usage, then:
 Now please don’t use this to go and bash your well-meaning dentist and hygienist, or the Arestin company, or worst of all, to justify the reasons you tell yourself why you don’t go to the dentist ’cause it’s all one big scam and you can’t trust anyone. Most of us really do want the best for you.
Now please don’t use this to go and bash your well-meaning dentist and hygienist, or the Arestin company, or worst of all, to justify the reasons you tell yourself why you don’t go to the dentist ’cause it’s all one big scam and you can’t trust anyone. Most of us really do want the best for you.
The point is simply this: if more people understand the difference between dental care that is patient-centered and dental care that is profit-centered, then greedy dental corporations are less likely to thrive.
If you think you have ever had this happen to you, I wrote this story for you. For you, so that you don’t feel so dumbfounded the next time you wonder whether or not a dental office is looking out for your health or only for their own. As a hygienist who knows fraud when I see it, I wanted to be sure that patients have a resource to help them defend themselves against predatory practices.
I’d like to end this with a small confession, then: I actually love placing Arestin, because when the dentist and I decide that it’s a good fit for a stubborn case of gum disease, it just feels so right.
So much for being objective.
![]()
References and resources:
Explanation of insurance coding of Arestin therapy after initial SRP: http://www.practicebooster.com
An example of Arestin-based fraud in a DHMO: http://caldentalplans.org/downloads/Henderson.pdf
Arestin drug label and study that shows slight improvement of using Arestin with SRP vs. SRP alone: http://dailymed.nlm.nih.gov/arestin
Criticism of Arestin studies and concerns about Arestin therapy : http://periodontist.org/is-arestin-a-therapeutic-treatment-for-reducing-gum-pockets/
 A blogger since 1997, Trish Walraven, RDH, BSDH is a practicing dental hygienist and marketing manager for an indie dental software development company. Her mission with DentalBuzz is to offer a fresh podium of discourse for those involved in dentistry and to expose fun in our professional lives.
A blogger since 1997, Trish Walraven, RDH, BSDH is a practicing dental hygienist and marketing manager for an indie dental software development company. Her mission with DentalBuzz is to offer a fresh podium of discourse for those involved in dentistry and to expose fun in our professional lives.