Don’t you think that this is the WORST part of orthodontia? You take off the brackets and voila! Straight teeth… with fugly white squares where acid beat the $#!† out your patients’ anteriors. And NOW you have to go drill on their teeth, destroying what you so carefully tried to perfect.
Once you’re here there’s no use in blaming the patient; it’s not like they’re going to get the brackets put back on to cover the white spots and then get more decalcification there. Yes, you should help them with their lifestyle choices (less energy drinks and voluntary mouth breathing, please) but at this point you have to do something to make them look better.
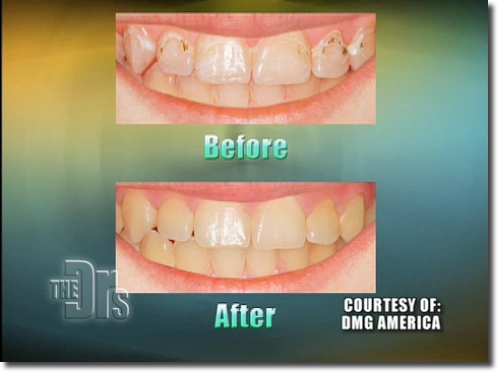
As a hygienist I’ve been totally itching for about the last four years to get the go-ahead to use a relatively new product called an infiltrant. There’s only one, it’s made by DMG and it’s called Icon. This infiltrant is placed on the tooth where it seeps into smooth-surface lesions that haven’t fully cavitated (although if you ask me the ones in the “Before” picture above look way gnarled out) and pretty much does a little remineralization voodoo.
I’d hoped that it would be classified as a sealant because Yay! I can do sealants. There’s no drilling done, right? There’s nothing taken away, right? There is, however, some irreversible improvement made to the tooth though and that (plus a significant etch time) means that when the CDT recognized that an infiltrant needed a code, where did that boom fall? Smack dab into Composite Land as a D2990. I know. The wording says “placement of an infiltrating resin restoration for strengthening, stabilizing and/or limiting progression of the lesion” and that SCREAMS prevention. Alas there’s the other word. Restoration.
Dangit.
Another problem is that this stuff is very expensive. See what it costs here for the mini kit for a maximum of six lesions?

That’s at best, $27 per tooth just for the kit (not including your other overhead or minusing the limited-time Amex card!). The suggested cost to a patient should be somewhere between your one surface composite fee and a sealant fee, and conservatively it takes at least 20 minutes of intense doctor time to place an infiltrant on a single tooth. Composites don’t cost that much or take that long to place so you know what that means, right? THE FEASIBILITY OF ICON SUCKS.
I really hope I’m wrong, but to most doctors, what’s a few millimeters of drilled-away tooth structure? Minimally invasive dentistry is for anal retentive freak dentists anyway. And every hygienist who has ever had a passion for preserving tooth structure, including me.
So yeah, this is bad news for Icon and for DMG, really. Sure, they got a CDT code this year but it’s not like anyone is going to use it. There’s like one dentist in a 5o mile radius that’s even ordered it around here. I know this because you can look on the DMG patient portal here and find a dentist that offers Icon in your area.
I have a challenge then. Actually two challenges – one for dentists, and the other for those who want to see this service added to the hygienist’s scope of practice in every state.
•If you’re a dentist and you love saving teeth, JUST DO THIS. Charge what you must, you’re not going to get rich, but you will have the warm fuzzy feeling that you’re doing the right thing by preserving tooth structure. We all know composites and amalgams eventually fail around their margins. There are no margins with an infiltration, just a lovely, arrested half-moon where an incipient lesion never progressed if you follow up with radiographs two decades from now (I may be exaggerating, but maybe not!). Go here, learn more, buy some.
•Those of you who are frustrated with dental hygienists wanting to become these mid-level providers that are supposed to help in low-access areas but will probably just come take your job away from you (I keed! I keed!) please support the use of infiltrants by hygienists. You will still need to diagnose that the treatment is needed but the service should be able to be delegated because of the very nature of the care being provided and the labor intensity needed for this smaller ROI.
As a realist, I don’t see squat happening as a result of this challenge. What can one blogger do? I have these silly dream glasses, when I put them on and see the future, well, there are no more cavities, on anyone, except arrested ones, and all the dentists are happy because all they have to do is play on the computer and nod their head every so often while their hygienists prevent all dental infirmities for ever and ever. Then I take them off again, and I see white spot lesions on teeth.
And I say…..dangit.
![]()
